What Might Cause A Bunion?
Overview
 A bunion is a very common foot deformity that develops over the first metatarsal phalageal joint of the big toe of the foot. The joint that joins the big toe to the foot is called the first MTP joint. When it becomes prominent and the big toe starts to become crooked this is known as a bunion. The term referring to deformity of the big toe as it becomes crooked is called Hallux Valgus. It is the bump itself that is known as the bunion. When it gets red and swollen over the bunion because it gets sore this is usually due to an inflamed soft tissue over the underlying bone.
A bunion is a very common foot deformity that develops over the first metatarsal phalageal joint of the big toe of the foot. The joint that joins the big toe to the foot is called the first MTP joint. When it becomes prominent and the big toe starts to become crooked this is known as a bunion. The term referring to deformity of the big toe as it becomes crooked is called Hallux Valgus. It is the bump itself that is known as the bunion. When it gets red and swollen over the bunion because it gets sore this is usually due to an inflamed soft tissue over the underlying bone.
Causes
Bunions have a number of causes, primarily genetics and bad choices in footwear. We inherit traits like flat feet, abnormal bone structure, and loose ligaments and tendons from our parents. When our feet are weakened by these traits and we stuff them into high heels or shoes which don?t support our feet correctly, the repeated stress on the front of the foot may contribute to the formation of a bunion. Other contributing factors are jobs that demand a lot of time standing, obesity, and sudden hormonal changes and weight gain, as in pregnancy. Unfortunately, bunions can lead to many other foot conditions as well. The joint behind the big toe carries much of your body weight and when the bunion makes it sore, you shift your weight onto other areas of the foot. That?s why we frequently see crossover toes, overlapping toes, hammer toes, corns, calluses, and ingrown toenails accompanying bunions. As pain in your foot increases, you?ll also reduce your activity, becoming more sedentary, which has its own quality-of-life issues.
Symptoms
Bunions may or may not cause symptoms. A frequent symptom is foot pain in the involved area when walking or wearing shoes; rest relieves this pain. A bunion causes enlargement of the base of the big toe and is usually associated with positioning of the big toe toward the smaller toes. Shoe pressure in this area can cause interment pain while the development of arthritis in more severe bunions can lead to chronic pain. Bunions that cause marked pain are often associated with swelling of the soft tissues, redness, and local tenderness. It is important to note that, in postpubertal men and postmenopausal women, pain at the base of the big toe can be caused by gout and gouty arthritis that is similar to the pain caused by bunions.
Diagnosis
People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen.
Non Surgical Treatment
Treatment of hallux valgus nearly always starts with adapting shoe wear to fit the foot. In the early stages of hallux valgus, converting from a shoe with a pointed toe to a shoe with a wide forefoot (or toe box) may arrest the progression of the deformity. Since the pain that arises from the bunion is due to pressure from the shoe, treatment focuses on removing the pressure that the shoe exerts on the deformity. Wider shoes reduce the pressure on the bunion. Bunion pads may reduce pressure and rubbing from the shoe. There are also numerous devices, such as toe spacers, that attempt to splint the big toe and reverse the deforming forces. 
Surgical Treatment
The most simple procedure is reducing the bump, and while there will be a little pain and swelling afterwards and your mobility will be restricted, the recovery time is short (ie a few weeks), but it may not fix the underlying cause. More serious ops might involve lasers, robots, cutting bone in the foot and trying to reposition it, and/or inserting pins or wires. It can take months to recover fully and you might need a cast. Mike O?Neill recommends seeking an NHS consultant surgeon who specialises in bunion removal to ensure the best possible outcome. The type of anaesthetic, local or general, will depend on the procedure, but most are day cases and the surgery will take from less than 30 minutes to a couple of hours. Waiting times vary but from your first outpatient appointment to the op would be a minimum of a few months. Private treatment (preferably by an NHS consultant surgeon) is likely to cost thousands of pounds. A new less, invasive procedure called surgical correction of hallux valgus that makes a small incision in the bone has recently been approved for use in the NHS but there is still no conclusive evidence on how effective it is and it is not widely available.
Prevention
If you are genetically at risk, not a lot. But shoes that are too narrow, too tight (even ballet flats) or have very high heels that force your toes down into the pointed end are asking for trouble. Aim for a 1cm gap between your toes and the end of your shoes. This doesn?t mean wearing frumpy flatties, the Society of Podiatrists and Chiropodists recommends sticking to 4cm heels for everyday wear, and wearing different types of shoe to vary the position of your foot. Gladiator styles can help because the straps stop your foot pushing down into the point of the shoe, ditto Mary Janes (sorry but for beautiful feet they need to have a strap), and flat, wide-fitting brogues are a no-brainer. Alternatively, in summer you can wear flip-flops to keep the space between your big and second toe as wide as possible. If you have children it?s vital to make sure that their feet are measured for properly fitting shoes to nip any potential problems in the bud. Keeping your feet and lower legs supple and strong is important too, that?s how A-list celebs get away with wearing killer heels, they all work-out like crazy. Exercises like trying to widen the space between your big toe and the second one with your foot flat on the floor, a few times a day can help, as can calf stretches. If you are devoted to any exercise that involves high impact for your feet, it might be worth checking that your gait and shoes are correct with a specialist shop such as Runners Need, as poor styles can cause irreparable bunion-related problems that will consign your trainers to the back of the cupboard for ever.
What Causes Overpronation Of The Foot
Overview
Overpronation still continues to be misused and misunderstood. For example, there was a study that got a lot of recent mileage in the mainstream media and the blogosphere that claimed to show that foot pronation was not associated with injury risk. It was intriguing following comments on the study in mainstream media and in social media, especially the parroting of the press release without any critical appraisal. The study actually eliminated the ?overpronators? that were probably at high risk from the study then found that ?overpronation? was not a risk factor. What is more intriguing was that there was another study from around the same time that found the exact opposite. Clearly, the data on ?overpronation? and risk for injury in runners is mixed, so we need to rely on the more formal systematic reviews and meta-analyses of all the data. The most recent one of those concluded that ?overpronation? is just a small risk factor for running injury risk, but it is still statistically significant.
Causes
Over-pronation may happen because the tissue that attaches to your foot bones is loose. You may be born with this problem or it may result from injuries or overuse, like from too much running.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Side Step with Opposite Reach. This exercise is designed to load the "bungee cord system" of the gluteal muscle and its opposite, latissimus dorsi muscle to keep the foot from overpronating. Because the opposite arm swings across the front leg when walking, this exercise creates tension in the muscles all the way from the front foot, across the back of the hips and back, to the fingers of the opposite hand. Movement Directions. Stand with left foot on top of the dome of the BT. (Note: For added balance, the right foot can tap on the ground, if needed). Reach right leg out to the side of the BT, and tap the ground while squatting down on the left side and reaching right arm across the left knee. Push down with left big toe while squatting. This activates the arch of the left foot and strengthens all the stabilizing muscles on the left side of the lower body. Return to starting position. Perform 8 to 10 repetitions on each leg.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Overpronation still continues to be misused and misunderstood. For example, there was a study that got a lot of recent mileage in the mainstream media and the blogosphere that claimed to show that foot pronation was not associated with injury risk. It was intriguing following comments on the study in mainstream media and in social media, especially the parroting of the press release without any critical appraisal. The study actually eliminated the ?overpronators? that were probably at high risk from the study then found that ?overpronation? was not a risk factor. What is more intriguing was that there was another study from around the same time that found the exact opposite. Clearly, the data on ?overpronation? and risk for injury in runners is mixed, so we need to rely on the more formal systematic reviews and meta-analyses of all the data. The most recent one of those concluded that ?overpronation? is just a small risk factor for running injury risk, but it is still statistically significant.
Causes
Over-pronation may happen because the tissue that attaches to your foot bones is loose. You may be born with this problem or it may result from injuries or overuse, like from too much running.
Symptoms
Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Side Step with Opposite Reach. This exercise is designed to load the "bungee cord system" of the gluteal muscle and its opposite, latissimus dorsi muscle to keep the foot from overpronating. Because the opposite arm swings across the front leg when walking, this exercise creates tension in the muscles all the way from the front foot, across the back of the hips and back, to the fingers of the opposite hand. Movement Directions. Stand with left foot on top of the dome of the BT. (Note: For added balance, the right foot can tap on the ground, if needed). Reach right leg out to the side of the BT, and tap the ground while squatting down on the left side and reaching right arm across the left knee. Push down with left big toe while squatting. This activates the arch of the left foot and strengthens all the stabilizing muscles on the left side of the lower body. Return to starting position. Perform 8 to 10 repetitions on each leg.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Calcaneal Apophysitis In Youngsters
Overview
During a growth spurt, your child?s heel bone grows faster than the muscles, tendons, and ligaments in her leg. In fact, the heel is one of your child?s first body parts to reach full adult size. When the muscles and tendons can?t grow fast enough to keep up, they are stretched too tight. If your child is very active, especially if she plays a sport that involves a lot of running and jumping on hard surfaces (such as soccer, basketball, or gymnastics), it can put extra strain on her already overstretched tendons. This leads to swelling and pain at the point where the tendons attach to the growing part of her heel.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
The most obvious sign of Sever's disease is pain or tenderness in one or both heels, usually at the back. The pain also might extend to the sides and bottom of the heel, ending near the arch of the foot. A child also may have these related problems, swelling and redness in the heel, difficulty walking, discomfort or stiffness in the feet upon awaking, discomfort when the heel is squeezed on both sides, an unusual walk, such as walking with a limp or on tiptoes to avoid putting pressure on the heel. Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
During a growth spurt, your child?s heel bone grows faster than the muscles, tendons, and ligaments in her leg. In fact, the heel is one of your child?s first body parts to reach full adult size. When the muscles and tendons can?t grow fast enough to keep up, they are stretched too tight. If your child is very active, especially if she plays a sport that involves a lot of running and jumping on hard surfaces (such as soccer, basketball, or gymnastics), it can put extra strain on her already overstretched tendons. This leads to swelling and pain at the point where the tendons attach to the growing part of her heel.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
The most obvious sign of Sever's disease is pain or tenderness in one or both heels, usually at the back. The pain also might extend to the sides and bottom of the heel, ending near the arch of the foot. A child also may have these related problems, swelling and redness in the heel, difficulty walking, discomfort or stiffness in the feet upon awaking, discomfort when the heel is squeezed on both sides, an unusual walk, such as walking with a limp or on tiptoes to avoid putting pressure on the heel. Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage.
Non Surgical Treatment
The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Causes Of Acquired Flat Foot
Overview
Adult acquired flatfoot is one of the most common problems affecting the foot and ankle. Treatment ranges from nonsurgical methods, such as orthotics and braces to surgery. Your doctor will create a treatment plan for you based on what is causing your AAFD. 
Causes
There are a number of theories as to why the tendon becomes inflamed and stops working. It may be related to the poor blood supply within the tendon. Increasing age, inflammatory arthritis, diabetes and obesity have been found to be causes.
Symptoms
Pain and swelling around the inside aspect of the ankle initially. Later, the arch of the foot may fall (foot becomes flat), this change leads to walking to become difficult and painful, as well as standing for long periods. As the flat foot becomes established, pain may progress to the outer part of the ankle. Eventually, arthritis may develop.
Diagnosis
Observe forefoot to hindfoot alignment. Do this with the patient sitting and the heel in neutral, and also with the patient standing. I like to put blocks under the forefoot with the heel in neutral to see how much forefoot correction is necessary to help hold the hindfoot position. One last note is to check all joints for stiffness. In cases of prolonged PTTD or coalition, rigid deformity is present and one must carefully check the joints of the midfoot and hindfoot for stiffness and arthritis in the surgical pre-planning.
Non surgical Treatment
Nonoperative treatment of stage 1 and 2 acquired adult flatfoot deformity can be successful. General components of the treatment include the use of comfort shoes. Activity modification to avoid exacerbating activities. Weight loss if indicated. Specific components of treatment that over time can lead to marked improvement in symptoms include a high repetition, low resistance strengthening program. Appropriate bracing or a medial longitudinal arch support. If the posterior tibial tendon is intact, a series of exercises aimed at strengthening the elongated and dysfunctional tendon complex can be successful. In stage 2 deformities, this is combined with an ankle brace for a period of 2-3 months until the symptoms resolve. At this point, the patient is transitioned to an orthotic insert which may help to support the arch. In patients with stage 1 deformity it may be possible to use an arch support immediately. 
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Pain In The Foot's Arch Triggers Signs And Symptoms And Treatment Options
Overview
The plantar fascia is a sturdy structure but the degree of stress that it takes makes it susceptible to injury. A force equal to almost three times body weight passes through the foot with each step. On running, this typically happens about 90 times a minute. Plantar fasciitis is thought to be a traction and overuse injury. Damage to the plantar fascia is usually in the form of micro-tears. It is a degenerative rather than an inflammatory process. Damage tends to occur near the heel, where stress on the fibres is greatest, and where the fascia is the thinnest. The fascia broadens as it extends toward the toes.
Plantar fasciitis is often associated with calcaneal spurs. These are depositions of calcium where the fascia suffers most damage. Spurs are most commonly on the medial side at the origin of the fascia from the calcaneum. Spurs are the result of the process of plantar fasciitis and not the cause of the pain. It can present bilaterally.

Causes
Also known as pes planus, this is when the arch of the foot collapses completely dropping the whole sole of the foot down to the ground. Flat feet are a common cause of foot arch pain. Babies are born with flat feet and as they grow, the foot arches should gradually form, but in approximately 30% of the population, they never do. They can also develop later in life, due to illness, pregnancy, injury, excessive stress on the feet or as part of the aging process. Many people who have flat feet don?t complain of any accompanying symptoms, but some develop foot arch pain, or problems further up the leg such as knee pain or back pain. They may find their feet tire quickly when they are standing or walking, and that it is difficult to rise up onto their tiptoes. Someone who is experiencing pain on the bottom of the foot or elsewhere due to their flat feet can benefit from exercises and orthotics (specially designed insoles to correct the foot position) as well as walking barefoot rather than in shoes. A quick test to see if you have flat feet is to put your foot in a tray of water and then place it on a smooth level surface e.g. thick paper. Have a look at your footprint, the more of the sole of the foot that you can see, the flatter your foot.
Symptoms
The foot of a newborn with congenital vertical talus typically has a convex rocker-bottom shape. This is sometimes combined with an actual fold in the middle of the foot. The rare person who is diagnosed at an older age often has a "peg-leg" gait, poor balance and heavy calluses on the soles where the arch would normally be. If a child with congenital vertical talus has a genetic disorder, additional symptoms often are seen in other parts of the body.
Diagnosis
In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics.
Non Surgical Treatment
The treatment of a rigid flatfoot depends on its cause. Congenital vertical talus. Your doctor may suggest a trial of serial casting. The foot is placed in a cast and the cast is changed frequently to reposition the foot gradually. However, this generally has a low success rate. Most people ultimately need surgery to correct the problem. Tarsal coalition. Treatment depends on your age, extent of bone fusion and severity of symptoms. For milder cases, your doctor may recommend nonsurgical treatment with shoe inserts, wrapping of the foot with supportive straps or temporarily immobilizing the foot in a cast. For more severe cases, surgery is necessary to relieve pain and improve the flexibility of the foot. Lateral subtalar dislocation. The goal is to move the dislocated bone back into place as soon as possible. If there is no open wound, the doctor may push the bone back into proper alignment without making an incision. Anesthesia is usually given before this treatment. Once this is accomplished, a short leg cast must be worn for about four weeks to help stabilize the joint permanently. About 15% to 20% of people with lateral subtalar dislocation must be treated with surgery to reposition the dislocated bone.

Surgical Treatment
Surgical advances have dramatically improved the ability to alleviate the pain and decreased function that millions of Americans experience due to flat feet. Nevertheless, many patients and even some physicians remain unaware of the new procedures, which are best performed by a foot and ankle specialist who has the applicable training and experience.
Prevention
The best method for preventing plantar fasciitis is stretching. The plantar fascia can be stretched by grabbing the toes, pulling the foot upward and holding for 15 seconds. To stretch the calf muscles, place hands on a wall and drop affected leg back into a lunge step while keeping the heel of the back leg down. Keep the back knee straight for one stretch and then bend the knee slightly to stretch a deeper muscle in the calf. Hold stretch for 15 seconds and repeat three times.
The plantar fascia is a sturdy structure but the degree of stress that it takes makes it susceptible to injury. A force equal to almost three times body weight passes through the foot with each step. On running, this typically happens about 90 times a minute. Plantar fasciitis is thought to be a traction and overuse injury. Damage to the plantar fascia is usually in the form of micro-tears. It is a degenerative rather than an inflammatory process. Damage tends to occur near the heel, where stress on the fibres is greatest, and where the fascia is the thinnest. The fascia broadens as it extends toward the toes.
Plantar fasciitis is often associated with calcaneal spurs. These are depositions of calcium where the fascia suffers most damage. Spurs are most commonly on the medial side at the origin of the fascia from the calcaneum. Spurs are the result of the process of plantar fasciitis and not the cause of the pain. It can present bilaterally.
Causes
Also known as pes planus, this is when the arch of the foot collapses completely dropping the whole sole of the foot down to the ground. Flat feet are a common cause of foot arch pain. Babies are born with flat feet and as they grow, the foot arches should gradually form, but in approximately 30% of the population, they never do. They can also develop later in life, due to illness, pregnancy, injury, excessive stress on the feet or as part of the aging process. Many people who have flat feet don?t complain of any accompanying symptoms, but some develop foot arch pain, or problems further up the leg such as knee pain or back pain. They may find their feet tire quickly when they are standing or walking, and that it is difficult to rise up onto their tiptoes. Someone who is experiencing pain on the bottom of the foot or elsewhere due to their flat feet can benefit from exercises and orthotics (specially designed insoles to correct the foot position) as well as walking barefoot rather than in shoes. A quick test to see if you have flat feet is to put your foot in a tray of water and then place it on a smooth level surface e.g. thick paper. Have a look at your footprint, the more of the sole of the foot that you can see, the flatter your foot.
Symptoms
The foot of a newborn with congenital vertical talus typically has a convex rocker-bottom shape. This is sometimes combined with an actual fold in the middle of the foot. The rare person who is diagnosed at an older age often has a "peg-leg" gait, poor balance and heavy calluses on the soles where the arch would normally be. If a child with congenital vertical talus has a genetic disorder, additional symptoms often are seen in other parts of the body.
Diagnosis
In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics.
Non Surgical Treatment
The treatment of a rigid flatfoot depends on its cause. Congenital vertical talus. Your doctor may suggest a trial of serial casting. The foot is placed in a cast and the cast is changed frequently to reposition the foot gradually. However, this generally has a low success rate. Most people ultimately need surgery to correct the problem. Tarsal coalition. Treatment depends on your age, extent of bone fusion and severity of symptoms. For milder cases, your doctor may recommend nonsurgical treatment with shoe inserts, wrapping of the foot with supportive straps or temporarily immobilizing the foot in a cast. For more severe cases, surgery is necessary to relieve pain and improve the flexibility of the foot. Lateral subtalar dislocation. The goal is to move the dislocated bone back into place as soon as possible. If there is no open wound, the doctor may push the bone back into proper alignment without making an incision. Anesthesia is usually given before this treatment. Once this is accomplished, a short leg cast must be worn for about four weeks to help stabilize the joint permanently. About 15% to 20% of people with lateral subtalar dislocation must be treated with surgery to reposition the dislocated bone.
Surgical Treatment
Surgical advances have dramatically improved the ability to alleviate the pain and decreased function that millions of Americans experience due to flat feet. Nevertheless, many patients and even some physicians remain unaware of the new procedures, which are best performed by a foot and ankle specialist who has the applicable training and experience.
Prevention
The best method for preventing plantar fasciitis is stretching. The plantar fascia can be stretched by grabbing the toes, pulling the foot upward and holding for 15 seconds. To stretch the calf muscles, place hands on a wall and drop affected leg back into a lunge step while keeping the heel of the back leg down. Keep the back knee straight for one stretch and then bend the knee slightly to stretch a deeper muscle in the calf. Hold stretch for 15 seconds and repeat three times.
What'S Adult Aquired FlatFoot ?
Overview
Adult acquired flatfoot deformity (AAFD) is a painful, chronic condition found most often in women between the ages of 40 and 60. AAFD occurs when the soft tissues of the foot are overstretched and torn, causing the arch to collapse. Flatfoot deformities may also be caused by a foot fracture, or may result from long-term arthritis. Once the posterior tibial tendon-the tendon unit that holds up the arch-loses its function, the foot becomes ?flat? as the bones spread out of position during weight bearing. Without an AAFD repair, the condition may progress until the affected foot becomes entirely rigid and quite painful. 
Causes
The cause of posterior tibial tendon insufficiency is not completely understood. The condition commonly does not start from one acute trauma but is a process of gradual degeneration of the soft tissues supporting the medial (inner) side of the foot. It is most often associated with a foot that started out somewhat flat or pronated (rolled inward). This type of foot places more stress on the medial soft tissue structures, which include the posterior tibial tendon and ligaments on the inner side of the foot. Children nearly fully grown can end up with flat feet, the majority of which are no problem. However, if the deformity is severe enough it can cause significant functional limitations at that age and later on if soft tissue failure occurs. Also, young adults with normally aligned feet can acutely injure their posterior tibial tendon from a trauma and not develop deformity. The degenerative condition in patients beyond their twenties is different from the acute injuries in young patients or adolescent deformities, where progression of deformity is likely to occur.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Observation by a skilled foot clinician and a hands-on evaluation of the foot and ankle is the most accurate diagnostic technique. Your Dallas foot doctor may have you do a walking examination (the most reliable way to check for the deformity). During walking, the affected foot appears more pronated and deformed. Your podiatrist may do muscle testing to look for strength deficiencies. During a single foot raise test, the foot doctor will ask you to rise up on the tip of your toes while keeping your unaffected foot off the ground. If your posterior tendon has been attenuated or ruptured, you will be unable to lift your heel off the floor. In less severe cases, it is possible to rise onto your toes, but your heel will not invert normally. X-rays are not always helpful as a diagnostic tool for Adult Flatfoot because both feet will generally demonstrate a deformity. MRI (magnetic resonance imaging) may show tendon injury and inflammation, but can?t always be relied on for a complete diagnosis. In most cases, a MRI is not necessary to diagnose a posterior tibial tendon injury. An ultrasound may also be used to confirm the deformity, but is usually not required for an initial diagnosis.
Non surgical Treatment
A painless flatfoot that does not hinder your ability to walk or wear shoes requires no special treatment or orthotic device. Other treatment options depend on the cause and progression of the flatfoot. Conservative treatment options include making shoe modifications. Using orthotic devices such as arch supports and custom-made orthoses. Taking nonsteroidal anti-inflammatory drugs such as ibuprofen to relieve pain. Using a short-leg walking cast or wearing a brace. Injecting a corticosteroid into the joint to relieve pain. Rest and ice. Physical therapy. In some cases, surgery may be needed to correct the problem. Surgical procedures can help reduce pain and improve bone alignment. 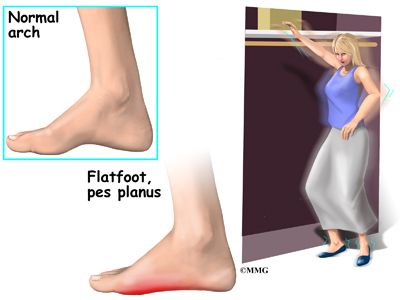
Surgical Treatment
For more chronic flatfoot pain, surgical intervention may be the best option. Barring other serious medical ailments, surgery is a good alternative for patients with a serious problem. There are two surgical options depending on a person?s physical condition, age and lifestyle. The first type of surgery involves repair of the PTT by transferring of a nearby tendon to help re-establish an arch and straighten out the foot. After this surgery, patients wear a non-weight bearing support boot for four to six weeks. The other surgery involves fusing of two or three bones in the hind foot below the ankle. While providing significant pain relief, this option does take away some hind foot side-to-side motion. Following surgery, patients are in a cast for three months. Surgery is an effective treatment to address adult-acquired flatfoot, but it can sometimes be avoided if foot issues are resolved early. That is why it is so important to seek help right away if you are feeling ankle pain. But perhaps the best way to keep from becoming flatfooted is to avoid the risk factors altogether. This means keeping your blood pressure, weight and diabetes in check.
Tips To Manage Pes Planus
Overview

Flatfoot (pes planus) is a condition that occurs when the arch or instep of the foot collapses or touches the standing surface. It is also known as fallen arches or pronation of the feet. The human foot is made up of 26 bones, 33 joints, and over 100 muscles, tendons and ligaments. The arch of the foot is created by tightening of the muscles and various ligaments that support the bones of the arch as well as ligaments that run from the heel to the ball of the foot. The arches distribute weight evenly across the feet and up the legs, and can affect walking. A well-developed arch is balanced between rigidity (for stability) and flexibility (for adapting to surfaces).
Causes
Genetic predisposition. Faulty foot mechanics, e.g. excessive pronation. Abnormal bony architecture. Laxity of ligaments. Neuro-muscular disease. Trauma to the leg muscles or major tendons. Inflammatory diseases of the joints e.g. Rheumatoid arthritis. Surgical procedures on the leg and ankle. Limb length inequality. Tight Achilles tendon.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms below. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks.
Non Surgical Treatment
Most cases of fallen arches are not painful and need no form of treatment. However, common symptoms of fallen arches can include pain in your feet (particularly in the area of your heel or arch), pain in your feet that persists after long bouts of physical activity or standing up, achy feet, or arch pain when standing on the tips of your toes. Most cases of fallen arches are not preventable. Treatments for fallen arches include, rest, ice, compression, medication to relieve pain, orthotics, or in some cases surgery.
Surgical Treatment

A combination of surgical procedures can be used to reconstruct the flatfoot. Generally, these procedures can be separated into those that correct deformities of the bones and those that repair ligaments and tendons. Your orthopaedic surgeon will choose the proper combination of procedures for your foot. Surgery of the foot can be performed under regional anesthesia, which is numbing the foot and ankle with a nerve or spinal block, or general anesthesia, which may require a breathing tube. A nerve block is often placed behind the knee to reduce pain after surgery.
Prevention
Flat feet or Fallen Arches cannot be prevented due to congenital of nature or from underlying disease process; however, painful symptoms and future pathology from Flat Feet or Fallen Arches may be prevented by the following. Continue to wear your orthotics for work and exercise to provide stability and maintain function of your feet. Footwear. Continue to wear supportive shoes to maximise the function of your orthotic and prevent excessive movement of the joints in your feet.
Flatfoot (pes planus) is a condition that occurs when the arch or instep of the foot collapses or touches the standing surface. It is also known as fallen arches or pronation of the feet. The human foot is made up of 26 bones, 33 joints, and over 100 muscles, tendons and ligaments. The arch of the foot is created by tightening of the muscles and various ligaments that support the bones of the arch as well as ligaments that run from the heel to the ball of the foot. The arches distribute weight evenly across the feet and up the legs, and can affect walking. A well-developed arch is balanced between rigidity (for stability) and flexibility (for adapting to surfaces).
Causes
Genetic predisposition. Faulty foot mechanics, e.g. excessive pronation. Abnormal bony architecture. Laxity of ligaments. Neuro-muscular disease. Trauma to the leg muscles or major tendons. Inflammatory diseases of the joints e.g. Rheumatoid arthritis. Surgical procedures on the leg and ankle. Limb length inequality. Tight Achilles tendon.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms below. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks.
Non Surgical Treatment
Most cases of fallen arches are not painful and need no form of treatment. However, common symptoms of fallen arches can include pain in your feet (particularly in the area of your heel or arch), pain in your feet that persists after long bouts of physical activity or standing up, achy feet, or arch pain when standing on the tips of your toes. Most cases of fallen arches are not preventable. Treatments for fallen arches include, rest, ice, compression, medication to relieve pain, orthotics, or in some cases surgery.
Surgical Treatment
A combination of surgical procedures can be used to reconstruct the flatfoot. Generally, these procedures can be separated into those that correct deformities of the bones and those that repair ligaments and tendons. Your orthopaedic surgeon will choose the proper combination of procedures for your foot. Surgery of the foot can be performed under regional anesthesia, which is numbing the foot and ankle with a nerve or spinal block, or general anesthesia, which may require a breathing tube. A nerve block is often placed behind the knee to reduce pain after surgery.
Prevention
Flat feet or Fallen Arches cannot be prevented due to congenital of nature or from underlying disease process; however, painful symptoms and future pathology from Flat Feet or Fallen Arches may be prevented by the following. Continue to wear your orthotics for work and exercise to provide stability and maintain function of your feet. Footwear. Continue to wear supportive shoes to maximise the function of your orthotic and prevent excessive movement of the joints in your feet.